
It is important for health information systems to talk to each other. Unfortunately they speak different languages. This article is not for eHealth experts to understand the nuances of interoperability (HIE), but for health care professionals to have an idea about what is out there and what can be expected in the future.
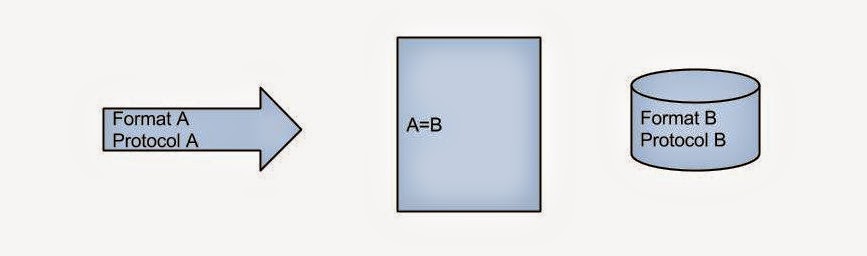
When we consider HIE we have to think about what is being exchanged (package), how the information is organized (format) and how it is being transported (protocol). Though it is not essential to know, few terms that you might recognize are: HL7, XML for format and HTTP, TCP/IP for protocol. (Have you heard of MLLP? Google it!) The donor has the information in a certain format and protocol while the recipient expects it in a particular format and protocol.

At the core of all HIE platforms such as MirthConnect or OrionHealth’s Rhapsody, is an engine that does this conversion. Format and protocol of donor to format and protocol of recipient. Simple eh?
Is pragmatic interoperability the best solution?- M. Martineau @eHealthMusings explores a pragmatic Rhapsody approach http://t.co/XMkMXAEdt7
— Orion Health Canada (@OrionHealthCA) December 11, 2014
Now most of these platforms have a user interface or IDE for making this connection. You can also introduce certain filters at this stage. Enterprise systems like Rhapsody presents an attractive visual interface, whereas open source solutions may not be very user friendly.
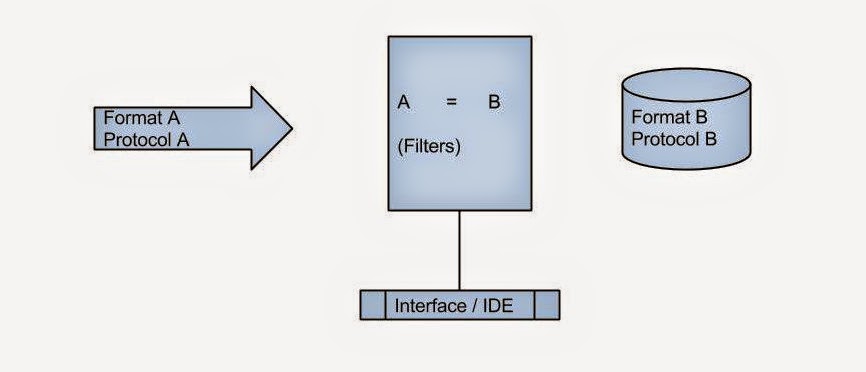
What else can the engine do? It usually keeps a log of all package deliveries and whether the delivery was successful. If the delivery failed, it can attempt again and alert the maintenance team through a console. The console can even be mobile as in rhapsody. Though the engine can store the package itself for a limited time, storing the package is not really its job.
The donors could be:
- A single department in a hospital sending lab reports.
- All departments in a hospital sending all sorts of information.
- Several hospitals in a region.
The recipient could be:
- Another department in the same hospital expecting a lab test report.
- A family physician who wants real time access to the lab reports for his patients admitted in the hospital.
- A researcher who wants to know blood sugar status of all the diabetes patients. (population health)
We need a separate layer between the engine and the recipient to support all these use cases. Let us call this layer mediator.
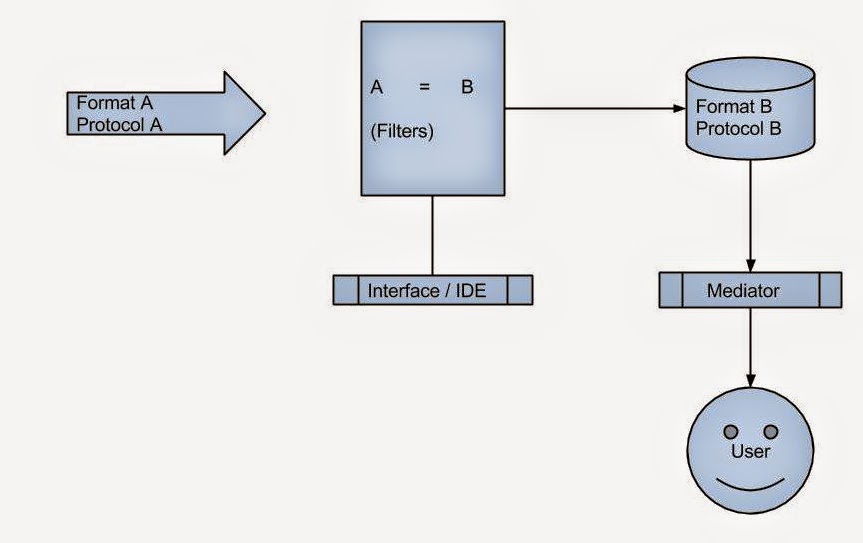
The mediator can pull data in real time from donors or store it in a local database. The first one is the federated model while the other one is the centralized model. Federated is slow but up-to-date while centralized is fast but not concurrent. Mixed model has both and is preferred. The so called clinical viewers are federated mediators with a web interface.
Emerging paradigms like NoSQL and RDF may be ideal for data representation in mixed model. I have discussed RDF before. Will discuss NoSQL soon!
- Word to LaTeX: How paperajcli Bridges Two Academic Worlds - May 5, 2026
- When GenAI Ideas translate to practice with DHTI - March 4, 2026
- How DHTI Makes MCP Practical for Healthcare Through “Docktor” (Part IV) - February 4, 2026
Brilliant!
Paper charts have been around for a century and their only purpose is to allow for communication between health care providers and institutions.
EMR/EHR and billing systems and mobile health devices because they have no standardization and integration or interoperability fail to allow providers and institutions to communicate and have only been proven to allow for enhanced billing due to default software content. Thus, software and hardware HIT systems in health care remain the only computer systems of any industry which don’t enhance the quality or cost of the products produced.
In addition to inhibiting communication amongst providers and insitutions, EMR/EHR and billing systems without integration and standardization fail to tabulate or reveal outcomes according to all their variables. These 4 outcomes (preventatitve, medical, surgical and palliative) are the only products manufactured or produced in health care. Without tabulation and revelation of outcomes, we in America will never know in real time who the best doctors and hospitals are or what the best diagnositcs and treatments are for which patients, we’ll remain empiric and retrospective.
The only industries which benefit by inhibiting interoperability via standardization and integration are the insurance, pharma, med mal, academe and EMR/EHR industry. Patients and doctors will continue to suffer due to this amazing lapse in technology.
Pingback: NoSQL in eHealth - NuChange
Pingback: Usability of Federated Clinical Viewers - NuChange